
INTRODUCTION
An injury resulting from external force is described as trauma. Children of today are facing this health problem a lot.1 Of all emergency visits, 15% of trauma involve teeth, periodontium and the supporting alveolar bone.2 The severity of trauma depends on the resistance of the tissues, the direction of impact and the energy of impact. The anterior region of the jaw is more susceptible for trauma.3 According to Gordy, children aged 6-15 years have higher incidence of injury to teeth and that they are serious as evidenced by high percentage of luxations, fractures, avulsions and dislocations.1 The dentoalveolar fractures may be present alone or may be associated with other injuries.4 Their cause can be attributed to playground accidents, bicycle accidents, fall, sports injuries and assaults.2 Although it may not leave significant scars on them but will defiantly have a psychological impact for sure.1 The successes of management of dentoalveolar injuries depends on proper diagnosis and prompt treatment within a limited time to achieve a favourable outcome, hence they should be treated as an emergency situation.2
The present article describes a simple technique of management of dentoalveolar fracture in a 7 year old boy with a follow up of 1 % years.
CASE REPORT
A 7 year old boy reported to the department of paedodontics and preventive dentistry with a history of trauma to the chin and anterior teeth because of fall while playing a swing. The patient was moderately built, cooperative and conscious. The patient presented with no history of loss of consciousness. On examination extra orally he had lacerations and swelling over the chin. Intra oral examination revealed that the patient was in early mixed dentition phase. There was a step deformity with deranged occlusion in the anterior segment of lower jaw. Tooth 72 showed grade 3 mobility. Contusion was seen in relation to lower labial mucosa (Figure 1 a).

|
Figure 1: (a) Trauma to mandibular anterior segment showing derangement of occlusion; (b) Cementation of open cap splint; (c) 1 / year follow up clinical photograph showing normal eruption of mandibular incisors.
Click here to view |
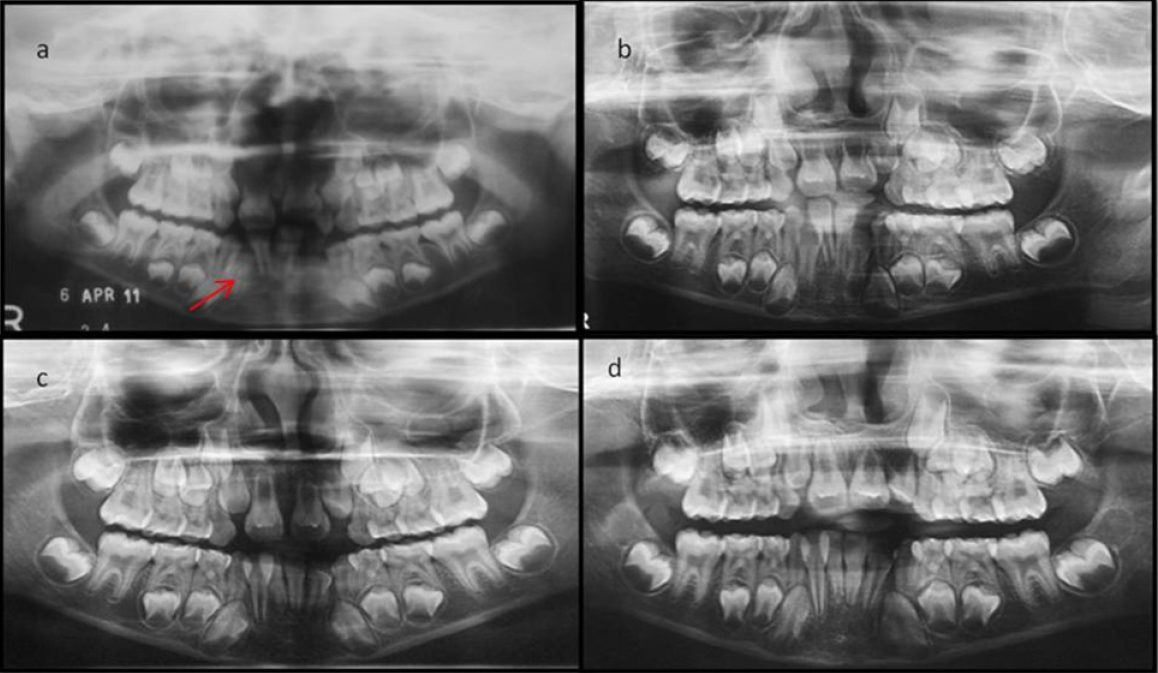
Orthopentomograph revealed a radiolucent line running distal and apical to 41 suggestive of dentoalveolar fracture (Figure 2 a). Hence an open cap splint was planned for the treatment. Under local anaesthesia alginate impressions of maxillary and mandibular arch made and casts were made by dental stone. Tooth 72 was extracted. Displaced mandibular segment was cut on the cast and stabilized with sticky wax and rearranged with the maxillary cast and the occlusion was re-established. A 19 gauge stainless steel wire was reinforced for the fabrication of open cap splint which was fabricated with self cure acrylic. After finishing and polishing the cap splint was tried in patient’s mouth after scaling and the occlusion was checked. Later the cap splint was cemented using zinc phosphate cement (Figure 1 b). The patient was advised to brush with soft bristles tooth brush and rinse with alcohol free chlorhexidine gluconate for 4 weeks. The cap splint was removed after 4 weeks. The healing was satisfactory except for mild inflammation of gingiva due to poor oral hygiene of the patient. The patient was advised at home oral hygiene instructions and was called for periodic recall every six months. Orthopentamograph was taken at every visit and the normal development of the permanent teeth in the mandibular anterior segment was evaluated (Figure 2 b, c and d). At 1 / year visit all the mandibular incisors had erupted and the radiograph showed continued root development (Figure 1 c).
|
Figure 2: (a) Orthopentamograph showing dentoalveolar fracture in lower anterior segment; (b) 6 month follow up; (c) 1 year follow up; (d) 1 ½ year follow up
Click here to view |
DISCUSSION
Due to less weight and small body size children are more vulnerable to any injury. Reports suggest that the incidence of facial trauma is more in males due to their risk taking and aggressive behaviour in preteen and adolescent age group. In any type of accident the maxillofacial region is the most common area to be injured due to its prominent anatomy. The injury in this region may have a temporary or permanent, partial or complete effect on mastication, speech and esthetics.5 These injuries have a profound effect in growth and development in the paediatric age group, hence the management has to be efficient in restoring the underlying bony architecture to its pre-injury position without damaging the underlying permanent tooth crypts .6
The dentoalveolar fracture can be effectively managed by closed reduction, immobilization and stabilization for 2-4 weeks.7 They can be manually reduced and stabilized with composite cement or wires and cap splints.8 The open cap splint offers many advantages besides being cost effective, simple and reliable, it offers better stability and also provides masticatory efficiency.9 Hence it was advocated in the present case. Also the paediatric patients have greater osteogenetic potential and accelerated healing compared to adults.9 Hence anatomic closed reduction can be considered in children.
CONCLUSION
Dentoalveolar trauma requires immediate care. Being a paediatric dentist conservative treatment has to be approached for this age group keeping in mind the anatomical complexity so as to attain a favourable outcome in the future growth and development of the child, which also has got an impact on the child’s psychology, aesthetics and function of mastication.