
INTRODUCTION
The soft palate is a movable muscular fold suspended from the posterior border of the hard palate.1 It separates the nasopharynx from the oropharynx and is often looked upon as traffic controller at the cross roads between the food and air passages. The palate controls the two gates the pharyngeal isthmus and the oropharyngeal isthmus. It can be completely close them or can regulate their size according to requirements.2 The main function of the palate are to direct the air flow to the nose and nasopharynx and direct the food bolus into the esophagus and prevent the nasal regurgitation of food and fluids thus it plays an important role in respiration and swallowing.3
The pre-maxilla or primitive palate is formed by the fusion of medial nasal folds which are folds of frontonasal process. The rest of the palate is formed by the shelf like palatine processes of the maxilla and horizontal plates of palatine bone. Most of the palate gets ossified to form hard palate. The unossified posterior part of the fused palatal process forms soft palate.4, 5 Various studies have been conducting for the dimensional analysis of the soft palate morphologies including its surrounding structures, but little attention has been paid to the varied soft palate morphology and configuration. You et al has classified the soft palate into six morphological varieties i.e. type 1: leaf shape or lanceolate; type 2: rat tail shape; type 3: butt shape; type 4: straight shape; type 5: S shape; type 6: Crook shaped.1
Pepin et al found that “hooked” shape of soft palate was in awake patients was associated with increased risk for obstructive sleep apnoea syndrome in which there is intermittent inspiratory closure of pharyngeal airway resulting in hypoxemia and sleep deprivation episodes.6 The hooked appearance was described as “S-Shaped” by You et al in their classification system.1 By determining the morphology of the soft palate in the lateral cephalogram it may be useful in determining the various morphological types in normal individuals. The aim of the present study was to determine the morphological varieties of the soft palate in normal individuals. The dimensional difference of the soft palate in relation to age and sex and the proportional differences in different age and gender groups were also studied in present study.
MATERIALS AND METHODS
A total of 202 digital lateral cephalograms recorded with the mandible in the position of maximal intercuspation were randomly taken in the department of oral medicine and Radiology. Lateral cephalograms were taken following a standradised method the age ranged from 6-50 years, including 131 males and 71 females. All the cephalograms were taken using digital orthopantomogram. The tube potential was adjusted to enhance the contrast of soft and hard tissues (80 kVp, 10 mA and 0.5sec). Digital radiographs were processed by Sidexes IX software All subjects who had normal speech function were selected. Patients with cleft lip and palate, history of trauma to the orofacial region, syndromic patients which involve craniofacial region were excluded from the study. The radiographs were analyzed and categorized by one radiologist into six types according to You et al and additional variety if present on two occasions.1 The two observations were carried out three weeks apart and matched. Intra examiner differences were evaluated and repeatability coefficient was above 0.9 for all variables thus confirming reliability of measurements.
The length of the soft palate was evaluated by measuring the linear distance from the posterior nasal spine (PNS) to the tip of the uvula of the resting soft palate.
All statistical procedures were performed using SPSS software. A cross-tab was constituted by dividing the subjects into two age groups preadults (below 18 years) and adults (above 18) in relation to the categories for comparing the constituent ratio between the two groups. The same procedure was followed when dividing subjects into male and female groups in relation to the categories for the same purpose. Tests were performed on both cross- tabs to evaluate for significant relationships among variables in the tables. Data of the velar length in each type are reported as mean + standard error (SE). One-way ANOVA (both least-significant difference test and Student Newman-Keuls test) was carried out to perform the multiple comparisons of the means between each two types.
RESULTS
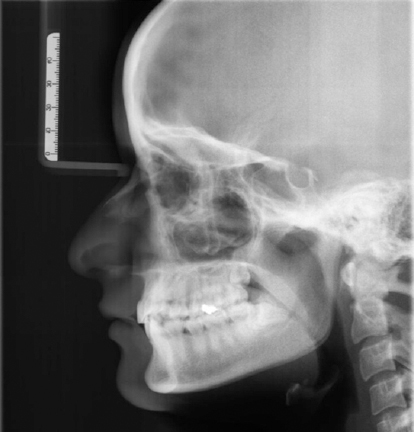
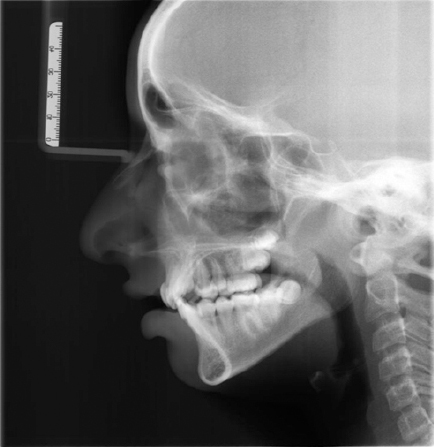
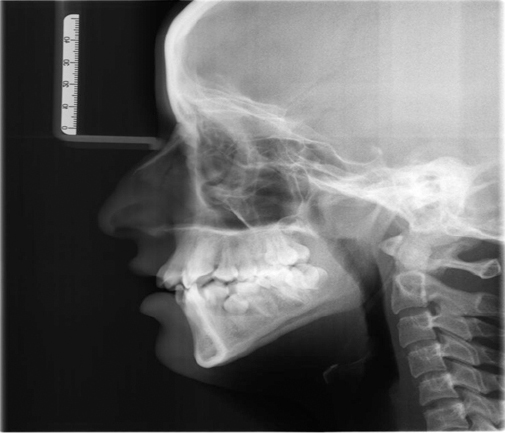
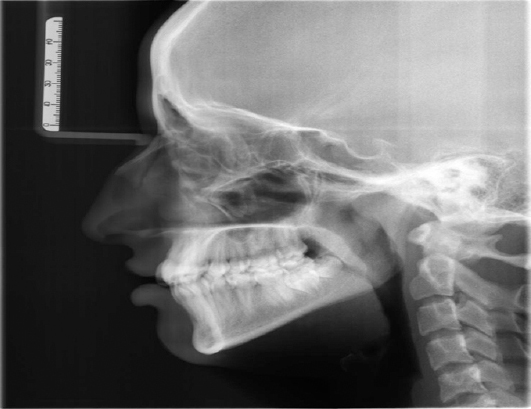
On observing the image of the soft palate on lateral cephalograms, we classified them into six types on the basis of the various radiographic appearances. The image and line drawing of each are given in Figures 1-6 and the results are tabulated (Tables 1-3).
|
Figure 1: Type 1 leaf shaped soft palate.
Click here to view |

|
Figure 2: Type 2 soft palate with rat tail shape.
Click here to view |
|
Figure 3: Type 3 soft palate with butt shaped.
Click here to view |
|
Figure 4: Type 4 soft palate morphology with straight line
Click here to view |
|
Figure 5: Type 5 soft palate with ’S’ shaped morphology
Click here to view |

|
Figure 6: Crook shaped in which soft palate curves anteriosuperiorly.
Click here to view |
|
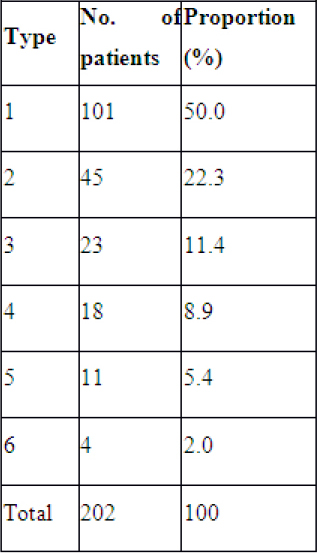
Table 1: Distribution aud proportio d of soft palate morphology types
Click here to view |
|
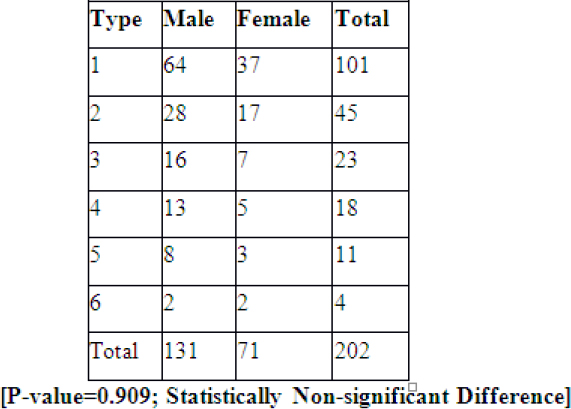
Table 2: Distributiou of soft palate morphology as per geuder
Click here to view |
|
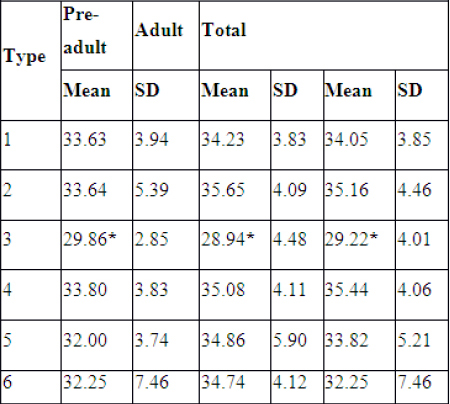
Table 3: Comparison of velar length in millimeters
Click here to view |
DISCUSSION
Soft palate function and development can be monitored and recorded by nasopharyngeal fibroscope and magnetic resonance imaging methods.7-10 However these methods are costly and are subjected to availability. Cephalometric analysis is commonly used to depict the soft palate morphologies in normal individuals and in cleft lip and palate patients. Cephalometry is a relatively inexpensive method and permits a good assessment of the soft tissue elements that define the soft palate and its surrounding structures.11
In the present study, the type 1 (leaf shaped) was the most frequent type (50% cases), noted in males and females, which was in accordance with the previous studies.1, 12, 13 This is the classic velar morphology of described earlier in the literature. Type 6 velar morphology was seen in only 1.5% cases.
In the current study, the velar length in Type 3 was significantly shorter than that in other types, but there was no significant difference between any two of the other five types. The significant shortness of Type 3 was also seen in both pre-adult and adult groups. The latter group may be thought to be more convincing, since the length of the soft palate is difficult to evaluate before adulthood.
According to age wise, subjects were distributed into two groups (preadults of less than 18years and adults of 18 years) and found statistically significant difference between the groups in their dimensions as there is potential possibility of growth of the soft palate as the individual grows, length of the soft palate increases and the morphologies of the some primary velar types changes. This is in concordance with various studies.1, 14-16
Obstructive sleep apnea is characterized by the recurrent occlusion of the upper airways resulting due to the inspiratory collapse of pharyngeal walls during sleep. Pepin et al found that a “hooked” morphology of the velum, which was described as “S-shaped” in our study, indicating high risk for obstructive sleep apnea in the awake patients. The hooking of the soft palate was defined as an angulation of 300 between the distal part of the uvula and the longitudinal axis of the velum. They hypothesized that soft palate hooking results in a sudden and major reduction in oropharyngeal dimensions, thus increasing the upper airway resistance and the transpharyngeal pressure gradient resulting in a pharyngeal collapse. The type 5 (S-shaped) soft palate was seen in 5.4% of the cases in the present study, while it was observed in 3.5% of the cases in the study of You et al and in 1.5% of the cases in Guttal et al studies.16
Kollias and Krogstad found that there is not statistically significant difference between the males and females in their length and thickness of the soft palate which is in concordance with our study. Praveen et al has also drawn the same results in their study.17
CONCLUSION
The morphology of the soft palate can be divided into six types according to their features on lateral cephalometry. This classification can help us to understand better, the diversity of the velar morphology in the median saggital plane. These findings can be used as references for the research of velopharyngeal closure in cleft palate individuals and for the etiological research of OSAS and other conditions.