
INTRODUCTION
Self injurious behaviour is the deliberatealteration to one’s own body part without suicidalintent.1, 2 Self inflicted injuries are common and canrange from simple to severe forms of mutilation. Many foreign objects are reported to be lodged inthe oral cavity like darning needles, pencil leads, metal screws, stapler pins and beads.3 Diagnosis offoreign bodies in the oral cavity is usually accidentalon clinical or radiographic examination and isusually associated with infection, pain andswelling.3-5
It becomes necessary to obtain a detailed casehistory along with clinical and radiographicexaminations to ascertain exact location, size, natureof the foreign body and difficulty encountered whileretrieving the foreign body. The present casedescribes the retrieval of a broken sewing needlefrom interdental area of teeth 74 and 75.
CASE REPORT
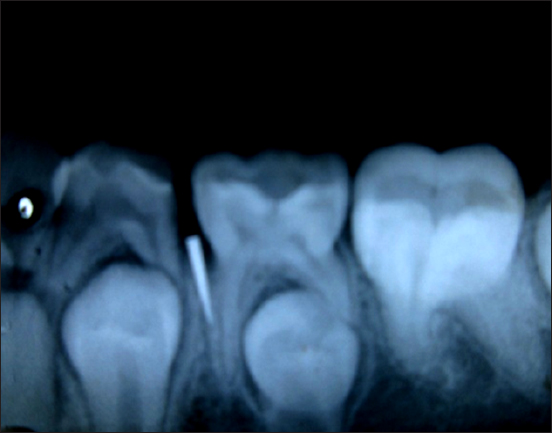
A 12 years old asian girl presented to theDepartment Of Pedodontics And PreventiveDentistry with a chief complaint of pain and foodlodgement in the lower left back region of jaw since 7 days. Intraoral examination revealed a proximalcarious lesion involving the distal surface of tooth74 and occlusal caries with 75 (Figure 1). The softtissue in the interdental area appeared normal. Anintraoral periapical radiograph was advised whichrevealed the presence of a sharp radiopaque objectpresent in relation to the interdental area betweentooth 74 and 75 (Figure 2). On further questioningthe child revealed to have used a needle which hadbroken in an attempt to take out the impacted food.

|
Figure 1: Mandibular arch showing distal caries with74 and occlusal caries with 75.
Click here to view |
|
Figure 2: IOPA showing radio opaque object in theinterdental area between tooth 74 and 75.
Click here to view |
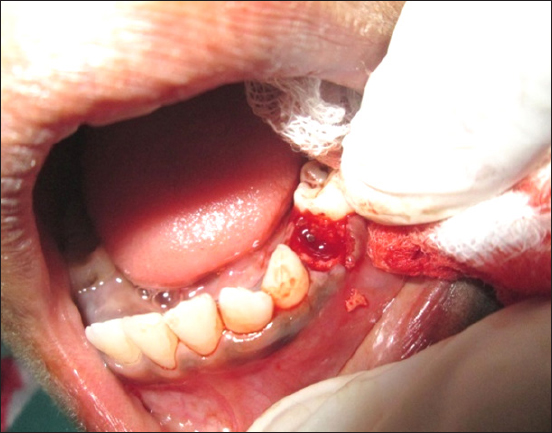
The procedure was explained to the child andparent; and informed consent was obtained. Extraction of tooth #74 was carried out under localanaesthesia. This provided vision and accessibilityfor the retrival of the broken needle from theinterdental area (Figure 3). On removal, thefragment measured approximately 8 mm in length(Figure 4). A post operative radiograph was taken toevaluate the complete removal (Figure 5). The patientwas followed up a week later when clinicalexamination revealed adequate healing and absenceof any pathology. Space maintainer was not plannedfor this patient since tooth 34 was in Nolla’s stage 7.
|
Figure 3: Needle fragment visible after extraction of tooth 74.
Click here to view |

|
Figure 4: Needle fragment after retrival.
Click here to view |

|
Figure 5: Post extraction IOPA
Click here to view |
DISCUSSION
One can inflict injuries to oneself owing tovarious activities like finger nail biting, bruxism, post-anaesthetic injury, to extreme self mutilationof oral mucosa. These injuries may be, unintentional, premediated or habitual and may be due to a widerange of organic functional or behaviouraletiologies.6
A radiograph plays a significant role indiagnosis, particularly if the foreign body isradiopaque. Various radiographic methods havebeen summarized by Hunter and Taljanovic tolocalize foreign objects such as vertex occlusal views, parallax views, triangulation techniques, tomography and stereo radiography. Metallic objectsare radiopaque unless made of aluminium.7, 8 In thepresent case it was accidental discovery with routineradiographic examination which was done toevaluate the carious lesion on the distal aspect oftooth 74. It helped in the exact location of the foreignobject.
McCullock suggested that access to foreignobject is improved by removing small amount oftooth structure. 3 In the present case since the needlewas not clinically visible and it was lodged deep intothe interdental area, extraction of the cariousprimary tooth was considered which showed morethan 2/3rd of distal root resorption which providedbetter visibility of the broken needle and thuspermitted easy removal.
CONCLUSION
The clinical behaviour in patients who have hada penetrating injury is determined by the nature ofthe impacted foreign body. Removal of the foreignbody becomes mandatory in most cases since theygenerally lead to secondary infection with abscessand eventually a formation of a fistula. Goldsteinhas reported a case of actinomycosis followingplacement of a jewellery chain piece into a maxillarycentral incisor.8 Apart from prevention of infection, it was necessary to remove the foreign body in thiscase as it was present interdentally and wouldinterfere with achieving proper contact of thesuccedeneous teeth.