
INTRODUCTION
Drug-induced gingival enlargement was firstreported in1939 by Kimball with chronic usage ofthe antiepileptic drug phenytoin.1 Currently, morethan 20 prescription medications are associated withgingival enlargement.2 Drug induced gingivalovergrowth may be due to hyperplasia of gingivalepithelium or of submucosal connective tissue or ofboth, the major drugs that causes gingivalhyperplasia are phenytoin (anti-convulsant), cyclosporine (immunosuppressant) and nifedipineand amlodipine (calcium channel blockers). Theyinteract with epithelial keratinocytes, fibroblastsand collagen, can lead to an overgrowth of gingivaltissue in susceptible individuals.3
Gingival hyperplasia is considered to be aserious adverse effect due to its unaestheticappearance and also due to its various complicationslike gingival bleeding, pain, teeth displacement andperiodontal disease.
Amlodipine is a new dihydropyridine calciumchannel blocker that is used in the management ofboth hypertension and angina. Ellis et al. firstreported gingival sequestration of amlodipine andamlodipine-induced gingival overgrowth.
Amlodipine is given in the dose of 5-10 mg oncedaily as it has a long duration of action. It is 93% -98% protein bound with a volume of distribution of21L/Kg. it is metabolized in liver to inactivemetabolite and is mainly excreted via urine.
Amlodipine has main action on vascular smoothmuscles It bind to the á-1subunit of L-type calciumchannels preferably on the vascular smooth muscles, block calcium entry and reverse vasospasm.
Pathogenesis
The pathogenesis of gingival overgrowth isuncertain and treatment is still largely limited tothe maintenance of an improved level of oral hygieneand surgical removal of the overgrowth tissues. Anumber of factors affect the relationship betweendrug and gingival overgrowth.
Role of fibroblasts
It has also been proposed that susceptibility orresistance to pharmacologically induced gingivalovergrowth may be governed by the existence ofdifferential proportions of fibroblast subsets in eachindividual which exhibit a fibrogenic response tothese medications. In support of this hypothesis, ithas been shown that functional heterogeneity existsin gingival fibroblasts in response to various stimuli.
Role of inflammatory cytokines
A synergistic enhancement of collagenousprotein synthesis by human gingival fibroblasts wasfound when these cells were simultaneously exposedto nifedipine and interleukin1b (IL1b), aproinflammatory cytokine that is elevated ininflamed gingival tissues. In addition to IL1b, IL6may play a role in the fibrogenic responses of thegingival to these medications. IL6 appears to targetconnective tissue cells such as fibroblasts both byenhancing proliferation and by exerting a positiveregulation on collagen and glycosaminoglycanssynthesis.21
Role of matrix metalloproteinase
Because most types of pharmacological agentsimplicated in gingival overgrowth have negativeeffects on calcium ion influx across cell membranes, it was postulated that such agents may interferewith the synthesis and function of collagenases.
Kantarci et al demonstrated that there aresignificantly higher numbers of basementmembrane discontinuities in overgrowth tissues, sometimes containing epitheliallike cells.17Disrupted basal membrane structure in gingivalovergrowth tissues is accompanied by adiscontinuous collagen type IV expression patternand decreased laminin5. These findings provided anew additional support for the hypothesis thatepithelial plasticity and epithelial to mesenchymaltransition promote gingival overgrowth, resultingin compromised basal membrane structure andincreased interactions between epithelial andconnective tissue layers that contribute to fibroticpathology.19, 20
Recently, Subramani et al observed that mastcells participate in many inflammatory oraldiseases, particularly those associated withfibrosis.21 They possess very diverse roles rangingfrom proinflammatory to immunomodulatory. Upontheir activation, they promote the local reninangiotensin system generation consequently able tostimulate endothelin and other profibroticmediators. Cyclosporin can modulate localexpression of renin angiotensin system componentssuch as angiotensinogen, angiotensin II and itsreceptors in gingival tissues, and gingival fibroblastcells.21, 22
MATERIALS AND METHODS
Potential subjects for this study were identifiedrandomly from the Department of Periodontology, of People’s Dental Academy, Bhanpur, Bhopal. Sixtyqualified individuals volunteered to participate inthe study. After obtaining written consent, aninterview and oral examination were performed oneach subject. The following parameters wererecorded: age; sex; Loe and Sillness Plaque Index, amlodipine dosage, duration and gingivalhyperplasia, using the grading system described byAngelopoulos and Goaz 1972 (Grade 0: No signs ofgingival enlargement, Grade 1: Enlargementconfined to interdental papilla, Grade 2:Enlargement involves papilla and marginal gingival, Grade 3: Enlargement involves three quarters ormore of the crown) (Figure 1, 2 and 3).

|
Figure 1 Amlodipine-induced Grade I enlargement
Click here to view |

|
Figure 2 Amlodipine-induced Grade II enlargement
Click here to view |

|
Figure 3 Amlodipine-induced Grade III enlargement
Click here to view |
Selection criteria included: 1) medication withamlodipine, 5 mg per day, for at least 6 months; 2)at least 10 natural teeth; 3) no other medicationknown to be associated with gingival hyperplasia;4) no antibiotic premedication required for dentaltreatment; and 5) no periodontal treatment withinthe previous 6 months.
Data Analysis
Chi-square test was used to determine anyrelationship of gender, drug dosage and durationwith gingival hyperplasia, and independent t-testanalyses were conducted to assess the role of age, plaque and gingival indices, by comparing groupswith and without gingival hyperplasia. Karl-Pearsoncorrelation coefficient between probing depth andgingival index score was also determined.
RESULTS
Overall results are presented in Table 1. Thirtyeight males and twenty two females, aged 31 to 79years, were examined. All subjects had been takingamlodipine for at least 6 months (mean duration:28 months), and all reported good compliance. Average Plaque indices 31%.

|
Table 1- sex, age range, plaque index, and Prevalence of Gingival Hyperplasia
Click here to view |
Mild gingival hyperplasia (score of 2) wasdetected in six subjects-a prevalence of 10%. Nocorrelations were found between gingivalhyperplasia and age, sex, duration of medication, or plaque index. While no statistically significantrelationship was found in this study between plaqueand hyperplasia. The most common dosage ofamlodipine is 5 mg per day and was chosen for thisstudy to facilitate obtaining a large sample size.
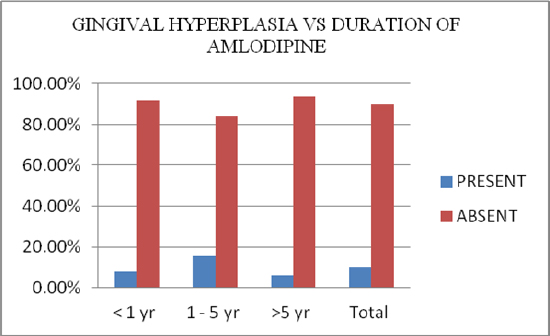
In summary, 60 dentate patients (38 males, 22females), 31 to 79 years of age, who had been takingamlodipine (5mg per day for at least 6 months), wereexamined for gingival hyperplasia (Graph 1). Moderate hyperplasia was detected in six patients-a prevalence rate of 10%, and association ofamlodipine induce gingival hyperplasia with age , sex , duration of medication and plaque index werefound to be statistically non-significant with pvalue>0.05.
|
Graph 1: Gingival hyperplasia and duration of amlodipine.
Click here to view |
DISCUSSION
Amlodipine is a 3rd generation dihydropyridinecalcium antagonist which is structurally similar tonifedipine but pharmacodynamically comparable toit. In patients with hypertensive heart disease theprevalence of gingival overgrowth associated withamlodipine is lower than that associated with othercalcium channel blocking agents includingnifedipine.6 Drug-induced gingival overgrowthusually occurs within the first 3 months of startingdrug therapy at a dose of 10mg/day and begins asan enlargement of the interdental papilla. Althoughfew cases of amlodipine induced hyperplasia havebeen reported, the present case is interesting as itoccurred with a low dose of amlodipine (5mg) andappeared on administration for 6 months.
Seymour et al.8 gave a review on thepathogenesis of drug-induced gingival overgrowthin which they considered it as amultifactorial model, involving an interaction of several factors, whichexpands on the interaction between drug andmetabolite with the gingival fibroblasts. Predisposing factors for these changes are age, genetic predisposition, pharmacokinetic variables, drug-induced alterations in gingival connectivetissue homeostasis, histopathology, ultrastructuralfactors and inflammatory changes, and drug-induced action on growth factors.
The underlying mechanism behind drug-induced gingival hyperplasia involves inflammatoryand noninflammatory pathways. The proposednoninflammatory mechanisms include defectivecollagenase activity due to decreased uptake of folicacid, blockage of aldosterone synthesis in adrenalcortex, and consequent feedback increase inadrenocorticotropic hormone level and upregulationof keratinocyte growth factor. Alternatively, inflammation may develop as a result of direct toxiceffects of concentrated drug in crevicular gingivalfluid and/or bacterial plagues. This inflammationcould lead to theupregulationof several cytokinefactors such as transforming growth factor-51. 9, 11
Many studies have been conducted whichshowed that amlodipine cannot induce gingivalhyperplasia at 5mg once daily dose even if taken formore than 6 months. It can be caused only at a doseof 10mg/day.6, 8 The present case is unique in thateven 5mg/day dose of amlodipine caused gingivalhyperplasia after 6 months of use.
The mechanism through which these drugsinduce gingival enlargement is still poorlyunderstood. It has been found that phenytoin andcalcium channel blockers inhibit the intracellularCa2+ uptake thereby stimulating gingivalfibroblasts. Not all the patients receiving the samedrug developgingival enlargement. Possible reasoncan be that individuals with gingival enlargementhave fibroblasts with an abnormal susceptibility tothe drug. It has also been proposed that thesusceptibility to pharmacologically induced gingivalenlargement may be governed by existence ofdifferential proportions of fibroblast subset in eachindividual which exhibit a fibrogenic response tothese medications. It has also been shown that thefunctional heterogenicity exists in gingivalfibroblasts in response to various stimuli.12
A synergestic enhancement of collagenousprotein synthesis by human gingival fibroblasts isfound when these cells are exposed simultaneouslyto calcium channel blockers and elevated levels ofinterleukin-15 (a proinflammatory cytokine) ininflamed gingival tissues. Interleukin-6 also playsa role in fibrogenic responses of gingiva to thesemedications. Interleukin-6 targets fibroblasts whichtrigger the proliferation of fibroblasts and exert thepositive regulation on collagen andglycosaminoglycans synthesis. So this cytokine hasbeen proposed to play a pathogenic role in fibroticgingival enlargement.8
Clinical relevant doses of cyclosporins triggergingival fibroblasts to exhibit significant reducedlevels of matrix metalloproteinases-1 and -3secretions which lead to accumulation ofextracellular matrix components.13 There is a strongcorrelation between the production of inactivecollagenase and responding fibroblasts. Because ofreduced folic acid uptake, there is limited productionof activator protein which converts inactivecollagenase to active collagenase. Limited amountof collagenase becomes available.8
Treatment consists of stopping the offendingdrug if possible with the patient’s physician consentand providing the supplements of folic acid andascorbic acid. Reduction in the size of the gingivalovergrowth has been reported within a week of drugwithdrawal and may lead to full resolution.14
Patients benefit from effective oral hygienemeasures, professional tooth cleaning, scaling, androot planning.15 If gingival enlargement persistsafter careful consideration of the previouslymentioned approaches, these cases need to betreated by surgery, either by gingivectomy or flapsurgery.
CONCLUSION
We conclude that the gingival hyperplasia couldoccur with amlodipine even at a small dose (5mg). Physicians and dentists should be aware of theetiologic medications that can induce gingivalhyperplasia and be able to identify changes in theoral cavity in such patients and to prevent, diagnose, and successfully manage them. It can be treatedlocally and systemically with combined effort ofmedical and dental physician. So, cooperativeteamwork between the patients, physician, and thedental health care professional is mandatory tominimize and successfully treat such unwanted sideeffects of drugs.